Stringy Clogs, Clumpy Milk, and Nipple Boogers
Trigger Warning: There is at least one graphic picture of a nipple that is not easy to look at.
“Why is my milk clumpy after pumping? It looked fine when I pumped it?”
“Why are there clogs stuck to my nipples after pumping?”
“Why do I have a clog that is stuck in my nipple pore and hurts to pull out?”
“Why is there a gross booger-like clog sticking out of that crack on my nipple?”
These are the ways that breastfeeding parents are describing what they see in their milk when pumping, and these descriptions are signs we need to evaluate for a possible breast infection. These are actual questions I have come across with clients, and I see variations of these questions in breastfeeding support groups all the time, particularly in pumping support groups. The root cause of the issues these parents are seeing is unrelated to pumping in itself, but pumping gives us a view of human milk that we simply don’t get with direct nursing.
Clogs can be a normal part of the breastfeeding experience. A milk duct can easily become blocked off due to a bad latch, a poor fitting bra, and any type of pressure against the breast. Sometimes, when these clogs are finally cleared we see the actual clog. But clogs should not be happening routinely, and when they are, you need to be evaluated by a lactation consultant to identify what is going on. Clogs are addressed by strategies such as heat, anti-inflammatories, correcting latches, and getting a good flange fit. Once we have addressed the issue, the clogs should not continue happening. When clogs continue to occur, we need to look into what is going on and consider the possibility of a breast infection.
This infection is referred to in three different ways in the literature: Subacute Mastitis, Subclinical Mastitis, and Mammary Dysbiosis.
These terms are interchangeable, and the differentiation seems to be that Subacute Mastitis and Subclinical Mastitis tend to appear in literature related to the dairy industry, where as Mammary Dysbiosis refers more to the clinical presentation in humans.
Is this infection different than what we commonly refer to as mastitis? Yes. Mastitis is actually a term that refers to the inflammation of the breast that is sometimes associated with an infection. You can follow this link here to learn everything you could have ever possibly wanted to know about Mastitis.
For the purpose of this discussion, we are going to use the term Mammary Dysbiosis as it more accurately describes what we are seeing. Mammary Dysbiosis is simply a descriptive term for the bacteria in the breast microbiome being out of balance (dysbiosis). This occurs when the bacteria in the breast associated with infections overgrows, and there is a lack of enough positive bacteria to keep it in check.
Signs and symptoms of Mammary Dysbiosis include:
Pain with the absence of clear trauma to the nipple
Trauma to the nipple that is slow to heal
Damage to the nipple of unexplained causes
High frequency of clogs
Frequent Milk Blebs
Tenderness of the breast with no clear origin
Nipple pain despite appropriate latch and pump flange fit
Milk that is clumpy after expression that appears normal when expressed, and has not been refrigerated to allow the milk fat to separate and solidify.
It’s important note that sometimes people present with no symptoms, limited symptoms or lots of symptoms. There is not one clear presentation of this infection, and it is often mistaken for other complications such as oral anatomy restrictions or thrush. Mammary Dysbiosis is, however, the overgrowth of bacteria.
Mammary Dysbiosis is a threat to breastfeeding continuation as often there is pain that is difficult to resolve without proper testing and labwork. It does not appear to be life threatening, and the course of untreated mammary dysbiosis is poorly understood. It will essentially follow one of three courses of action…
It will become an active infection that we recognize as mastitis, with warmth, redness, and pain that will be treated with antibiotics.
It will remain the same with pain persisting for a long period of time with no obvious signs of a classical infection.
The body will eventually fight off the overgrowth and balance will be restored to the breast causing resolution of pain.
Most commonly we identify this infection when we have a parent present with clumps in their milk. Watch the video below to see how the clumps in the milk for this mother, who was ultimately confirmed with labwork to have a coagulase positive breast infection (it literally causes the milk to coagulate at room temperature which is atypical for human milk.
With parents using the Willow Pump, we are seeing some curious presentations of Mammary Dysbiosis due to the way that the Willow Pump functions. With a traditional pump, the milk is rapidly moved from the nipple and into the bottle - milk doesn’t pool around the nipple. With the Willow Pump, milk is maintained in the flextube for a period of time until the flextube fills enough to trigger the pump to transfer the milk to the container or bag. This allows for milk to pool around the nipple for some time. We also have a higher incidence of the milk being kept in the bag for a period time, and even small clumps become more obvious when they stick to the sides of the Willow bag.
We are also seeing increased reporting of clogs being routinely pulled from the breast (remember, clogs like this aren’t normal, this shouldn’t be happening this frequently). In some cases, the coagulase action of the bacteria is happening when the nipple is being held in the milk, and we are actually getting clogs that form half outside of the nipple pore, and when the pump is removed, they are hanging out of the nipple. Because these are not formed in the same way as a regular milk fat clog, they actually end up dilating the nipple pore slightly and have to be manually pulled from the nipple. This can be very painful. In the cases where a nipple crack was present, this seems to provide a higher likelihood of these clogs forming. We get some clogs falling out of the crack best described as boob boogers due to the gelatinous nature of them.

See the tiny clog hanging out of the nipple? Its firmly embedded in the nipple pore and quite uncomfortable. Prior to this pump session there was no clog in the breast so to find a dislodged clog was abnormal.
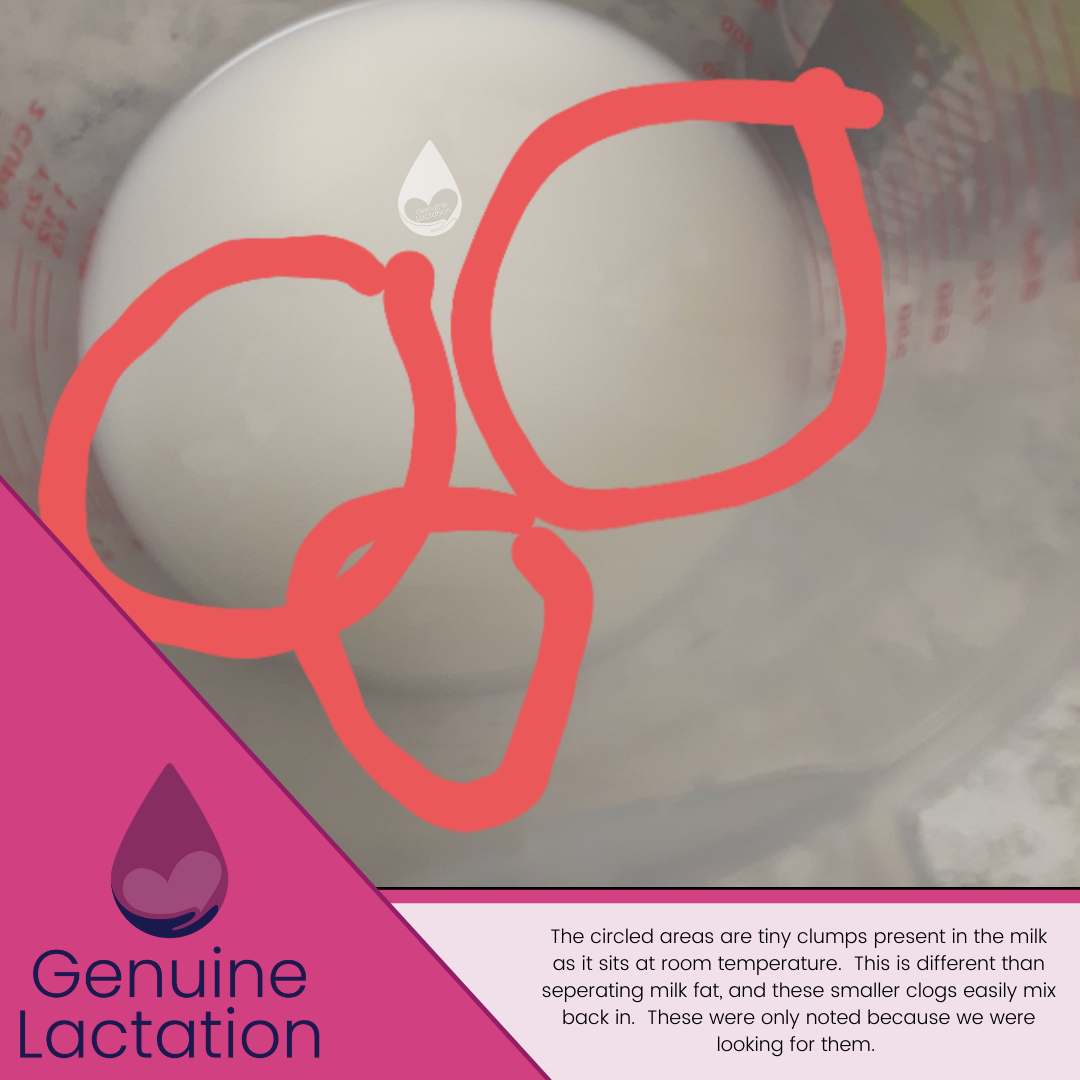
The circled areas show small discolorations in the milk, which were originally thought by the parent to be the separation of milk fat. The milk had not been refrigerated yet which is a red flag for clumps to be investigated.

Here you can see another clog that is too large to have come out of that nipple pore. With these clogs I am routinely getting reports that the clog seems to form outside in, and this is only being seen with the Willow Pump.

This clog formed on the outside of a nipple crack and was a clear indication that medical treatment was necessary. It was not from inside of the nipple, but the coagulase positive bacteria were clinging to the cut skin.
So what should you do if you are experiencing symptoms consistent with clumpy milk, indeterminate pain, nipple damage that is not healing, or milk clogs including those hanging off of the nipple? You need to see a lactation consultant ASAP to be evaluated. While you may ultimately also need to see a medical provider to address the issue thoroughly, you still need a full lactation work-up to rule out other causes and to assure your symptoms are ONLY from a possible case of Mammary Dysbiosis. Antibiotics won’t fix manual trauma, and fixing the latch or pump flange fit won’t cure a bacterial infection. True relief comes when we address all of these causes together.